
Health & Wellness: Understanding The Knee & Injury Prevention

For basketball players, really for any athlete at all, maintaining health and performing at peak physical condition is the most important thing to focus on, and a lot of the time, it’s probably that area of athletics which is most taken for granted. In this Health & Wellness section, I would like to focus on different joints, muscle groups, and nutrition specific to basketball, using scientific research and professional opinions from leading medical experts in the Midwest. I want to make these topics easily understandable for the average prospect, parent, and coach, so I will attempt to stray from medical jargon and do my best to keep everything in layman’s terms.
This specific article will focus on understanding the makeup of the knee, identifying five key components within the knee, and offering tips to help prevent injuries to one of the joints that is central to nearly all activities in basketball (i.e. running, jumping, sliding, stopping). I want to dispel any rumors you may have heard, because in my opinion, knee injuries often receive a lot of overreaction due to their long rehabilitation timeline, therefore too many uninformed people publicly offer their opinion with very little factual information to back it up. While this article isn’t intended to answer every question in relationship to knees and knee injuries, hopefully it will be informative and offer you something you weren’t previously aware of.
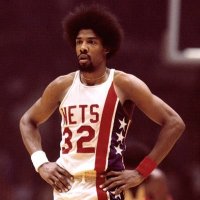
Picture courtesy of OrthoIllustrated.com
The Basics
While there are many more parts to the anatomy of the knee, the key terms you often hear are the ACL, the PCL, the MCL, the LCL, and parts of the Patellar region (the patellar tendon, the patella, and the quadriceps tendon). I will focus more on these specific items throughout this article.
The four core knee ligaments (ACL, PCL, MCL, LCL) are actually bundles of strands/fibers that are intertwined like a rope to form a sturdier band of tissue connecting the femur (upper leg) to the tibia (lower leg), stabilizing the knee region as a unit. While you can technically have a partial tear to one of those ligaments, it will eventually “unravel” or “fray” like a rope or piece of twine if part of it is severed. I have seen situations where a player crumples to the floor with very little force or movement, but if you go back to a point earlier in the game, they were possibly contacted by another player and it just took that long for the ligament(s) to eventually tear completely.
That’s why many orthopedics treat partial ACL tears like full tears, and they often recommend surgery, even if you’ve only partially torn your ACL. There are instances, though very rare, where you can rehabilitate a partially torn ACL without surgery, but in some cases the rehabilitation process can take longer and be more frustrating than having the surgery itself.
ACL (Anterior Cruciate Ligament)
The ACL and the PCL (detailed below) are a pair of ligaments arranged in a crossed formation through the center of the knee. They are attached to notches in the middle of the femur (upper leg) and the tibia (lower leg). The ACL, specifically, prevents the knee from going forward. For example, in a basketball setting, if you are running and you choose to jump-stop, the ACL will keep your knee’s momentum from carrying it forward and dislocating.
ACL tears are commonly caused by the knee suddenly rotating inward, causing the femur to move forward and the tibia to move backward (in opposite directions). Imagine the femur temporarily sliding over the tibia/shin before returning to its proper position. That’s a little bit of a crude example, but hopefully you get the point.
Females are actually more susceptible to ACL injuries for a variety of reasons. First, females often have wider hips, which can cause their knees to already bend inward. Second, females tend to have stronger quadriceps than hamstrings, and they rely on their quadriceps a lot more, adding more strain to the knee joint. Third, the combination of wider hips and stronger quadriceps causes a wider quadriceps angle, or Q-angle, which puts more strain on the knee joint. And fourth, females typically have smaller knee joints, shorter knee ligaments, and smaller notches in their femurs where the ACL and PCL connect, causing a higher level of strain on the knee joint.
Now, I’m not going to spend a lot of time talking about the different types of surgeries, etc., but I did want to briefly touch on the rehabilitation timeline if you are unfortunately diagnosed with an ACL injury. To begin with, there is no perfect, mathematical equation to figure out your recovery time, so a lot of what follows are approximations. There are many variables to recovery, including, but not limited to: your size (height and weight), the condition you were in pre-injury (muscular strength, muscular stamina), your work ethic, your commitment to the rehabilitation plan put in place by your doctors, your ability to mentally and emotionally overcome your injury and “jump back on the horse” when you’re released, and your resources (money, facilities, equipment, high school training staff).
Assuming you have the typical recovery of most athletes, the ACL should be fully healed in 6-8 weeks post-operation. This doesn’t mean you are ready to begin activities, it just means the ACL itself is now structurally sound. It’s likely going to be closer to 3½ to 4 months before you’ll be able to resume any activities. This doesn’t mean you’re ready to begin competition. This means non-contact drills, some jogging/running, and some light weightlifting, plus a lot of balance, bending, and stretching exercises.
If everything goes well to this point, it will take another 6-8 weeks of participating in activities on a regular basis to start regaining your old form. A lot of the time, this is where the process is taken for granted. Athletes think they’re either healed already, or they get lazy, and they won’t put in the consistency of activity necessary to continue the rehabilitation timeline as scheduled.
In total, you’re probably looking at anywhere from 6-9 months to begin playing in competition again, but sometimes, depending on the variables stated above, it can take as long as 12-14 months for you to begin feeling like yourself again and showing the same explosion/athleticism you had pre-injury. But, in many cases, your repaired ACL will be stronger than the initial, healthy ACL.
It is somewhat rare, but you can sprain your ACL just like you would sprain an ankle. It can be difficult to tell if you’ve simply sprained it (no tearing), because unlike an ankle injury, you can’t see or feel the swelling/bruising of an ACL on the surface of the skin since it runs through the middle of the knee. Really the only way to tell if you’ve sprained your ACL is through a series of MRI tests, but you might have to wait a few days after the injury for the swelling to go down to be sure. If it is diagnosed as a sprain, the rehabilitation period is approximately 4-6 weeks depending on your preexisting health and your commitment to sticking to a specific rehabilitation program.
PCL (Posterior Cruciate Ligament)
Like the ACL, the PCL is a ligament in the center of the knee. It also attaches to notches in the middle of the femur (upper leg) and the tibia (lower leg). The PCL is actually comprised of two bands though, not one like the ACL, therefore it is a bit stronger and “easier” to play through and rehabilitate if injured. The PCL prevents the knee from going backwards.
A lot of times, depending on the violent nature of an injury, the PCL is torn along with the ACL. While it is less-often damaged on its own than an ACL, it does happen from time to time. The primary causes of a PCL injury would be if you fell hard directly on the knee while it was bent in a 90-degree angle, or if you maybe get hit hard in the shin, and in both cases the knee is suddenly forced backwards.
The good news for a PCL injury by itself, is that in most situations surgery is not required. There will still be a rehabilitation period of roughly 4-6 weeks to allow for swelling to dissipate and for the ligament to begin healing and working at full strength again. But again, as mentioned with the ACL rehabilitation, you will still need to strictly follow your rehabilitation steps/assignments to stay on schedule.
MCL (Medial Collateral Ligament)
The MCL runs down the inside of your leg, and more specifically, it runs down the inside of the knee joint, connecting the femur and the tibia. The MCL can occasionally be injured on its own, especially in contact situations when the knee is slightly bent and buckles inward. But in most cases, the MCL is injured in conjunction with an ACL injury.
Rehabilitation of the MCL is actually separated into three categories: Grade-1, Grade-2, and Grade-3. For a Grade-1 MCL injury, which is more of a stretch/sprain than a tear, you are looking at just a few days to maybe a couple of weeks. For a Grade-2 injury, when your MCL is partially torn, the timeline can take as long as a month. And for a Grade-3 MCL injury, or a complete tear of the ligament, it can take two months or longer for it to completely heal.
LCL (Lateral Collateral Ligament)
The LCL runs down the outside of your leg, and more specifically, it runs down the outside of the knee joint, connecting the femur and the tibia. The LCL helps to protect the knee from buckling outward. Because of its location, and the amount of force it would take to cause this, it is extremely rare to injure your LCL without damage to another or multiple other ligaments in your knee. In fact, if you are diagnosed with just an LCL injury, due to the rarity of it being injured alone, it’s advised to ask your doctor to doublecheck both the ACL and the PCL once again to ensure there is no damage to either of those ligaments.
Rehabilitation of the LCL falls in line similarly to that of the MCL. It too is separated into different categories, or “Grades”, and the recovery time for the severity of the injury is nearly identical as well.
Patellar Region (Patellar Tendon/Patella/Quadriceps Tendon)
This is a real basic version of anatomy, but the quadriceps tendon connects to the quadriceps muscle group over the bottom of the femur (upper leg) on the front side of the leg. The quadriceps tendon then connects at the other end to the top of the patella (knee cap). The patellar tendon connects at one end to both the bottom of the patella and to the quadriceps tendon in order to hold the patella in place, and at the other end the patellar tendon connects to the top of the tibia on the front side of the leg.
Picture courtesy of wiktionary.orgNow, a patellar tendon tear is rare, but if it happens, it can be more severe than an ACL injury due to it stabilizing the entire front side of the knee on its own, plus helping to keep the patella in place, whereas the ACL, the PCL, the MCL, and the LCL work together to stabilize the middle of the knee joint. In most cases, though, people tend to heal completely from a patellar tendon tear with no structural issues, but not everyone will regain the full amount of strength in the tendon they had pre-injury.
An injury in this region that is common in females is called a patellar subluxation. This is when the patella quickly pops out of place and then back in on its own. It is often mistaken for a patellar dislocation, which is when the patella pops out of position entirely, even slides over to the side of the leg, and needs to be “reduced”, or popped back into place by a medical professional.
If the patella continues to pop in and out of place with regularity and becomes a major problem, then surgery is an option. If you’ve ever known anyone who has had shoulder surgery because their shoulder kept popping out of place, it’s very similar. The doctors will essentially go in and “tighten” the ligaments and tendons around the patella itself to better hold it in place. They do so by shortening the ligament to give the joint better support.
Knee Injury Prevention/Precautions
Unfortunately knee injuries are a part of sports, and there is no magical “cure” to avoid them entirely. While you can build strength, increase flexibility, and improve your nutrition, there’s nothing to prevent the “freak” injury. I mean, you could just as easily injure yourself walking down the stairs or slipping in the bathtub at home. There are, however, a few things you can do to lessen your chances of injury in sports, especially injuries that occur in non-contact situations.
– Probably the best preventative measure for knee injuries is to perform more functional activities. This means replicating movements and activities you would perform in normal game situations. Something as simple as getting in a lower, wider stance defensively, or being in a stance “ready to score” on every catch offensively can help, as long as it’s done on a consistent basis. Not that this is full-proof, but I’ve known teams who switched from zone defense to man defense, and as they began working on closeouts, slides, and stances a lot more, they saw their number of knee injuries decrease.
– The weight room is another tool that is either underutilized or misunderstood/misused. In theory, it seems like a great idea to occasionally get in the weight room and work out. But if your attendance is intermittent, if you aren’t performing lifts that will benefit you and your body, or if you aren’t using proper technique, then it’s almost better to avoid the weight room until you are ready to commit to it regularly and properly. It is OKAY to lift in-season. If you’re worried about fatigue, then stick to lifting light weight, but always lift with proper technique. Also, as it relates to females specifically, we discussed above that ladies tend to rely on their quadriceps too much and their hamstrings too little. Focus instead on lifts that help strengthen your hips, your core, your glutes, and your hamstring strength.
– There are also several activities you can do outside of the gym or the weight room. Proper and thorough stretching is a great start that comes to mind. I’m not talking about reach down and try to touch your toes for 10 seconds. I mean talk to a doctor or athletic trainer and find a nice 20 to 30-minute stretching routine that you can use to both stretch and strengthen your muscle groups. Incorporate resistance bands and medicine balls into your stretching as well. You can also add in a mixture of walking stretches, jumping exercises, and lunging exercises to that routine.
– Braces in general on any of your body’s joints are solid injury prevention devices, however understand when to use them and how to use them. THEY ARE NOT CURES!!! A lot of athletes who return from a knee injury are fully healthy, but emotionally they can’t move on without wearing a knee brace of some sort. If you didn’t wear a brace pre-injury, then it’s advised not to wear one post-operation, especially to get over that mental hurdle. If you are healthy, and you are strong, then allow your body to work on its own. However, if for example, you have weak ankles, a brace will help stabilize your ankle joint, but you’re still going to have weak ankles. You need to continue working on strengthening exercises to build up your ankle joint so you can perform with or without a brace, and the brace isn’t used as a crutch or an excuse for you not to work to build strength.
– I’ve been around several athletes who have torn their ACLs, and at some point in their recovery, or even once they are back competing again, they tear some of the scar tissue in their knee joint. Yes, there will be a little pain, and it will initially frighten you a little, as it should, but understand this can and likely will happen at least once in your recovery. In most cases the pain only persists for a few seconds, maybe a couple of minutes, but if all else is good after that, then that is probably what happened. It’s a nice little reminder of what you don’t want to happen again.
– With that in mind, re-tears will happen for a variety of reasons. Rarely does it ever mean your ACL itself wasn’t healed. If a re-tear happens within a few months after surgery or after being released, it’s often because an athlete rushed back to competition and didn’t fully strengthen the knee and the muscle groups around the knee. If it happens a year or more post-operation, then it can typically be attributed to any of the causes outlined above in the ACL section of this article. No matter what, though, none of us are immune to joint injuries, and we can’t prevent landing on someone’s foot awkwardly or having someone fall into our legs. Bizarre accidents happen in sports, especially in contact sports, and it’s just an unfortunate part of the game. But, if you ever find yourself in the position of having to rehabilitate a serious knee injury, be sure to STICK TO THE PLAN prescribed by your doctors, and follow it exactly as it is laid out for you. That’s the best way to ensure you will make a full recovery and are able to be back on the court as quickly as possible.
Special Thanks:
I would like to give a special thanks to John Darmelio, ATC-Retired, for his help and insight into this article. John currently serves as a Clinical Assistant to Doctor Thomas Klootwyk at Methodist Sports Medicine in Indianapolis/Carmel. Their orthopedic team specializes in knee reconstruction, arthroscopic knee surgery, and orthopedic sports medicine, and Dr. Klootwyk serves as one of the team physicians for the Indianapolis Colts of the National Football League. You may learn more about their practice at: www.methodistsports.com.
Header photo courtesy of t-nation.com.







")









